GLUTEUS MEDIUS & MINIMUS TRAINING – TRAINING RESEARCH
Click on Image to Enlarge
Weak Glute Medius-Minimus causes Hip Drop and Hip Internal Rotation stressing the Hip Joint, the Lateral Hip & the Knee
ULTRASOUND
GLUTEUS MEDIUS
– Aging
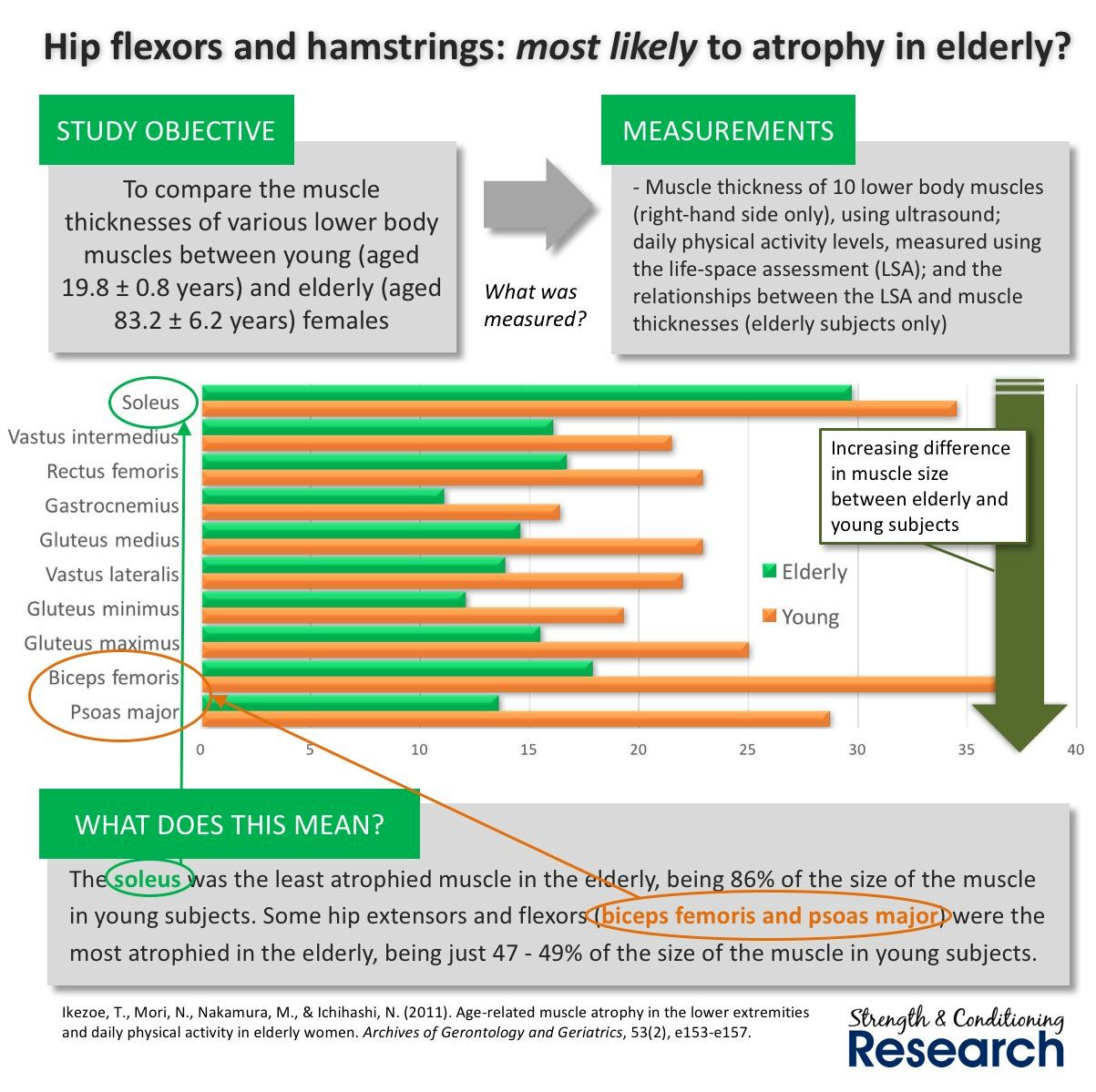
Age-related muscle atrophy in the lower extremities and daily physical activity in elderly women – 2011 – Ikezoe
Procedure
– relationship between age-related declines in muscle thickness of lower extremities daily physical activity in elderly women
– 20 young women and 17 elderly women residing in a nursing home
– Daily physical activity was evaluated using life-space assessment (LSA) which assessed degree of independence
– muscle thickness was measured by B-mode ultrasound
Results
– Only the G-Med was significantly associated with the LSA score
MOTION CAPTURE – GROUND REACTION FORCES – EMG
GLUTEUS MAXIMUS-MEDIUS-MINIMUS
– Multiple Exercises
Gluteal Muscle Forces during Hip-Focused Injury Prevention and Rehabilitation Exercises – Collings 2023
Procedure:
– 14 female footballers (18-32 yrs)
– at least 3 months of lower limb strength training experience
EMG STUDIES
GLUTEUS MEDIUS
– Multiple Exercises
Exploring the Role of the Lateral Gluteal Muscles in Running: Implications for Training – Fetters – 2020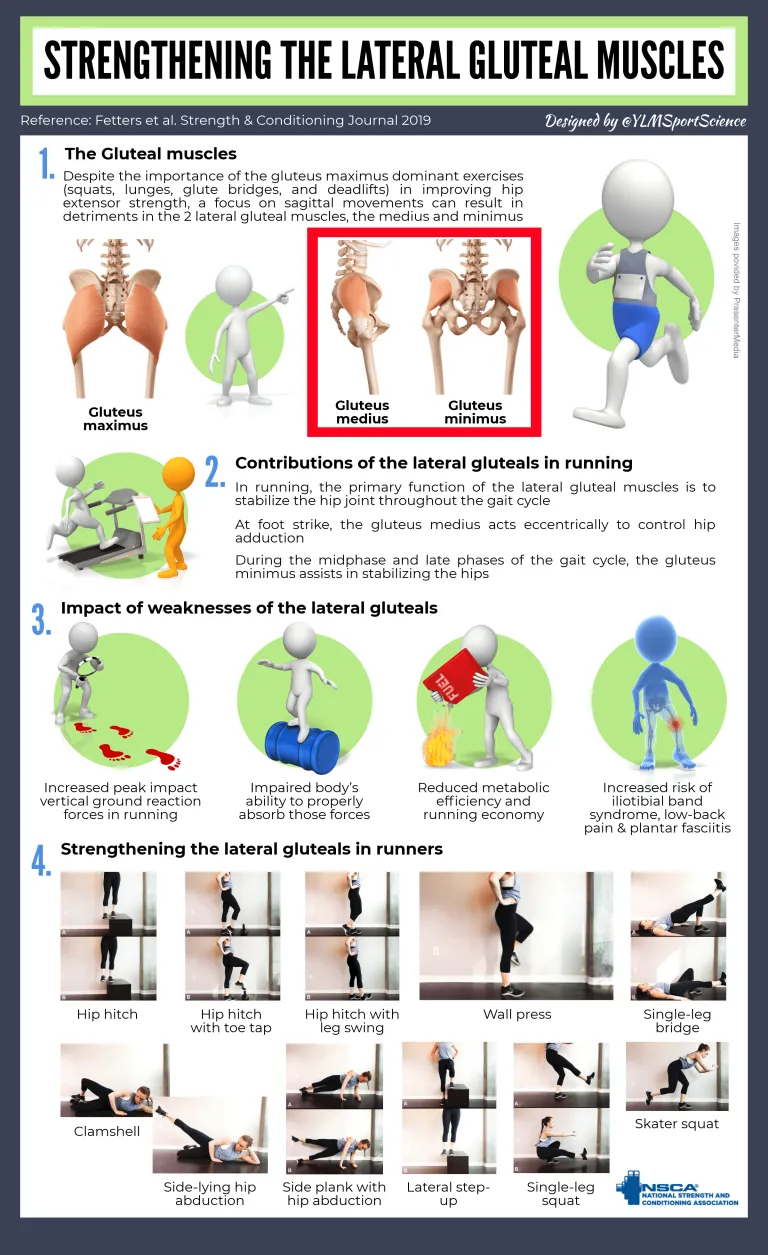
Exercises
– The hip hitch produces high levels of muscle activity in all sections of the G-Med and G-Min
– The single-leg bridge, clamshell and side-lying hip abduction produce high levels of the G-Med
– The side-lying hip abduction also elicits high levels of activation in the posterior segment of the G-Min
Running and other Dynamic Activity
– Compound resistance training exercises are important because running is a dynamic activity involving multi-joint movement
– Unilateral, closed-chain exercises are considered sports-specific to runners; lateral gluteals stabilize the hips during the single-leg stance phase of running
– Unilateral compound exercises like lateral step-up, single-leg squat, and skater squat produce high levels of G-Med activation
GLUTEUS MEDIUS
– Multiple Exercises
Gluteus Minimus and Medius Muscle Activity During Common Rehab Exercises in Healthy Postmenopausal Women – Ganderton – 2017
Exercises
– For single leg exercises participants placed one hand on a chair or the wall; testing non-stance leg
Hip Hitch . Toe Tap . Leg Swing . SHA – Standing Hip Ab-duction . Sit to Stand . Split Squat . Clam
Results
G-Med – Anterior: Swing 75 . Hitch 73. Toe Tap 70 . Split Squat 50 . SHA 40 . Sit to Stand 30 . Clam 5
G-Med – Middle: Swing 70 . Hitch 50. Toe Tap 40 . Split Squat 30 . SHA 30 . Sit to Stand 20 . Clam 10
G-Med – Posterior: Swing 60 . Hitch 50. Toe Tap 40 . Split Squat 35 . Sit to Stand 30 . Clam 30 . SHA 25
G-Min – Anterior: Hitch 60 . Swing 60 . Toe Tap 50 . SHA 45 . Split Squat 25 . Sit to Stand 15 . Clam 10
G-Min – Posterior: Swing 80 . Hitch 70. Toe Tap 70 . Split Squat 70 . SHA 40 . Sit to Stand 30 . Clam 10
GLUTEUS MEDIUS
– Multiple Exercises
Review and Analysis of Common Therapeutic Exercises that Generate Highest Muscle Activity for Glute Medius – Moore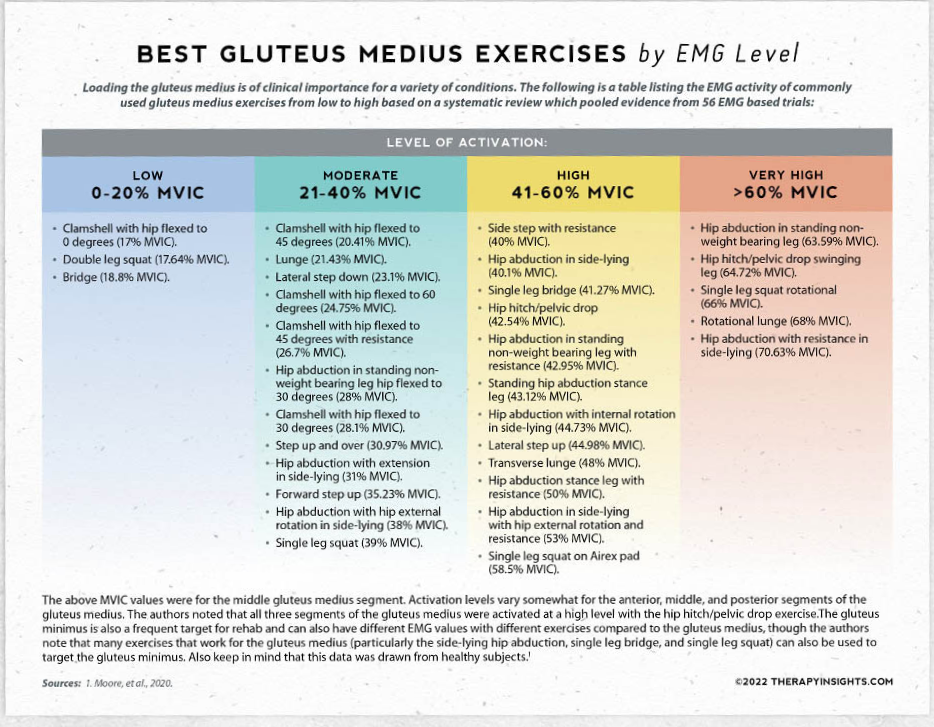
Introduction
– Evaluate high >40% MVIC EMG activity in the G-Med (anterior, middle and posterior)
Results for Stabilization Exercises
Hip Hitch and Pelvic Drop
– 8 Studies: Anterior 41%, Middle 43%, Posterior 43%
– 1 study with 3 variations of hip hitch/pelvic drop: Anterior 68-74%; Middle 41-65%; Posterior 45-60%
Step-ups Forward & Lateral – Middle G-Med
– 21 Studies: Forward Step-up = Middle 35%; Lateral step-up = Middle 45%
– Adding resistance to a Lateral Step-up = Middle 40%
– Wide Variations: technique; step height; step distance; concentric and eccentric phase; stepping or supporting leg measures; addition of external resistance
– 1 study: Anterior 88%, Middle 85%, Posterior 81% for the forward step up and over exercise
Lunge and Split Squat
– 10 Studies: Forward Lunge Middle 21% and Side lunge Middle 22%
– 1 study: measured rear-foot elevated lunge Bulgarians (dip test): Anterior 45%, Middle 71%, Posterior 28%
– There was some variation between the studies on lunge technique, active range of movement and movement plane
Single-Leg Squats
– 13 Studies: Middle 39%
– Large variations did however exist between the studies including squat depth, exercise technique and number of repetitions
– 1 Study: Anterior 90%, Middle 92%, Posterior 87%
– 1 Study: Single leg squat with isometric hip abduction and isometric hip adduction: middle 27-31%; posterior 22-33%; anterior 42% for isometric adduction, 19% for isometric abduction.
Single Leg Wall Squats
– 4 Studies: Middle 32%
– 1 Study: Single leg wall squat with isometric hip abduction or isometric hip adduction. Anterior 13-29% Posterior 28-44%
Squats with or without medial or lateral resistance, or wall support
– 6 studies: squats Middle 18%; squats with resisted abduction Middle 35%
Bridge: 7 studies
– 6 Studies: Single Leg Bridge Middle 41%
– 5 Studies: Double Leg Bridge Middle 19%
Standing Hip Ab-duction Stance Leg
– 2 Studies: Middle 43%
– 1 Study: Anterior 56%, Middle 30%, Posterior 41%
Results for Hip Ab-duction
Standing Hip Ab-duction Swing Leg
– 2 Studies: had added external resistance Middle 43%; There was however a high degree of heterogeneity.
– 1 Study: without added resistance recorded Middle 64%
Side-Lying Hip Ab-duction
– 8 Studies: Middle 40%; external resistance further increased activity levels to very high although there was a high degree of heterogeneity
– 4 Studies: Middle hip abduction with internal rotation 45%; hip abduction with external rotation 38%
Side-Lying Clams
– There were wide variations between studies for exercise technique; angle of hip and knee flexion; repetitions; and use of external loading
– 10 Studies: Middle 17-28%
– 1 Study: Anterior 3%; Middle 13%, Posterior 23%; Altering the angle of hip flexion or trunk position had minimal effect
GLUTEUS MEDIUS
– Multiple Exercises
EMG studies evaluating G-Max and G-Med activation during rehab exercises . Michael Reiman – 2011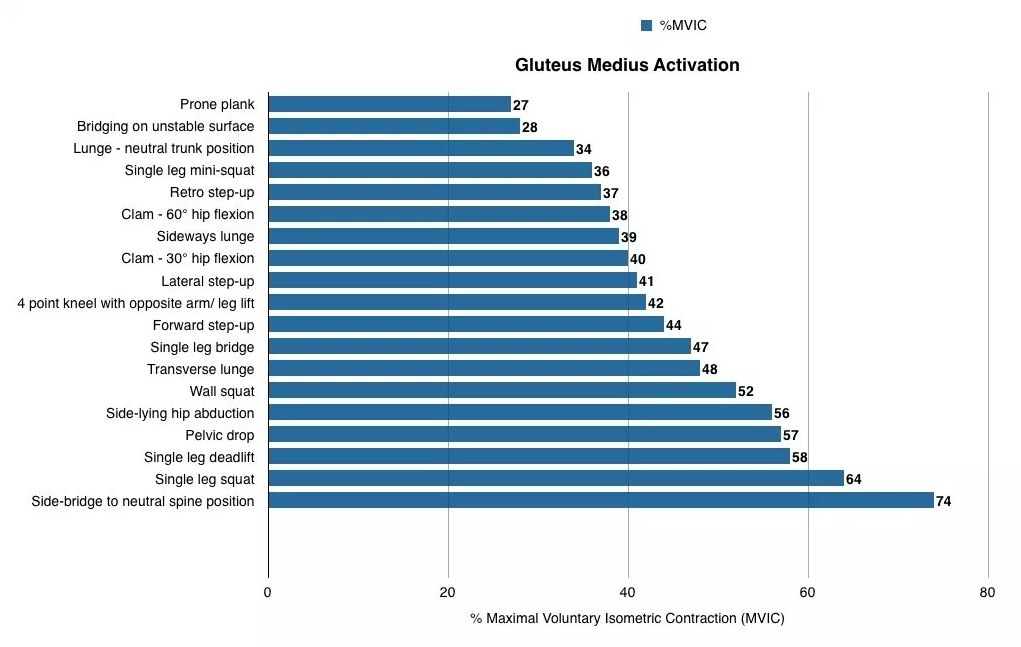
Procedure & Results for Gluteus Maximus
– Studies included evaluated activation of GMax during rehab exercises; subjects were healthy
– the following can affect EMG activity: (1) trunk position (2) movement direction (3) base of support
– strength gains are expected for activation levels = or >40% MVIC
· 74% – side bridge to neutral spine position
· 64% to 52% – 1-leg squat; 1-leg RDL; pelvic drop; side lying hip ab-duction; wall squat;
· 48% to 40% – transverse lunge; side leg bridge; forward step-up; bird dog; lateral stepup; clam 30º hip flexion
· 39% to 34% – sideways lunge; clam 60º hip flexion; retro backward stepup; single leg mini-squat (single leg 1/4 squat); lunge neutral trunk;
· 25% to 19% – bridging on unstable surface; prone plank
UPPER GLUTEUS MAXIMUS, GLUTEUS MEDIUS, TFL
– Multiple Exercises
Which Exercises Target the Gluteal Muscles While Minimizing Activation of the Tensor Fascia Lata? – 2013 – Selkowitz 
Procedure
– which exercises are best for GMed and superior portion of GMax, while minimizing activity of TFL
Fine Wire Electrodes
– Sup-Gmax: midpoint of line drawn b/n posterior superior iliac spine and posterior GT
– GMed: 2.5 cm distal to midpoint of iliac crest (ie, middle portion)
– TFL: distal and slightly lateral to anterior superior iliac spine and medial and superior to GT
Results
| Exercise | Tensor Fascia Lata | Gluteus Medius | Superior Gluteus Maximus |
|---|---|---|---|
| Side-lying hip abduction | 32.3 ± 13.1 | 43.5 ± 14.7 | 23.7 ± 15.3 |
| Bilateral bridge – Hip Thrust | 8.2 ± 7.4 | 15.0 ± 10.5 | 17.4 ± 11.9 |
| Clam | 11.4 ± 11.4 | 26.7 ± 18.0 | 43.6 ± 26.1 |
| Hip hike | 31.4 ± 14.4 | 37.7 ± 15.1) | 17.7 ± 15.2 |
| Lunge | 21.6 ± 14.5 | 19.3 ± 12.9 | 20.1 ± 11.1 |
| Quadruped hip ext, knee extending | 15.6 ± 9.3 | 27.3 ± 14.9 | 28.5 ± 16.6 |
| Quadruped hip ext, knee flexed | 18.7 ± 10.6 | 30.9 ± 15.2 | 30.1 ± 12.5 |
| Sidestep | 13.1 ± 7.1 | 30.2 ± 15.7 | 27.4 ± 16.7 |
| Squat | 4.6 ± 3.8 | 9.7 ± 7.3 | 12.9 ± 7.9 |
| Step-up | 21.4 ± 11.4 | 29.5 ± 14.9 | 22.8 ± 15.6 |
| Unilateral bridge – Hip Thrust | 18.1 ± 12.9 | 30.9 ± 20.7 | 34.6 ± 16.8 |
GLUTEUS MEDIUS
– Mini Squat, Wall Mini-Squat, Mini Step-down
Comparative Effects of 4 Single-Leg Squat Exercises in Subjects With Gluteus Medius Weakness – Han
Procedure & Results
– 22 subjects with GMed weakness (Note: leaning on the wall reduces activation)
G-Med: uni wall-squat 23% . lateral step-down: 22% . front step-down: 21% . uni squat: 20%
TFL: lateral step-down: 38% . front step-down: 35% . uni squat: 30% . uni wall-squat 25%
Ad-ductor Longus: uni wall-squat 25% . front step-down: 20% . lateral step-down: 18% . uni squat: 16%